

UNPRECEDENTED overall survival (OS) benefit with 1L KIMMTRAK3-9
Largest phase 3 trial in metastatic uveal melanoma (mUM) evaluated first-line treatment with KIMMTRAK vs investigator’s choice (IC)3,4
- Investigator’s choice included checkpoint inhibitors (pembrolizumab and ipilimumab) or chemotherapy (dacarbazine)3,4

HISTORIC 5-YEAR follow-up analysis of OS2
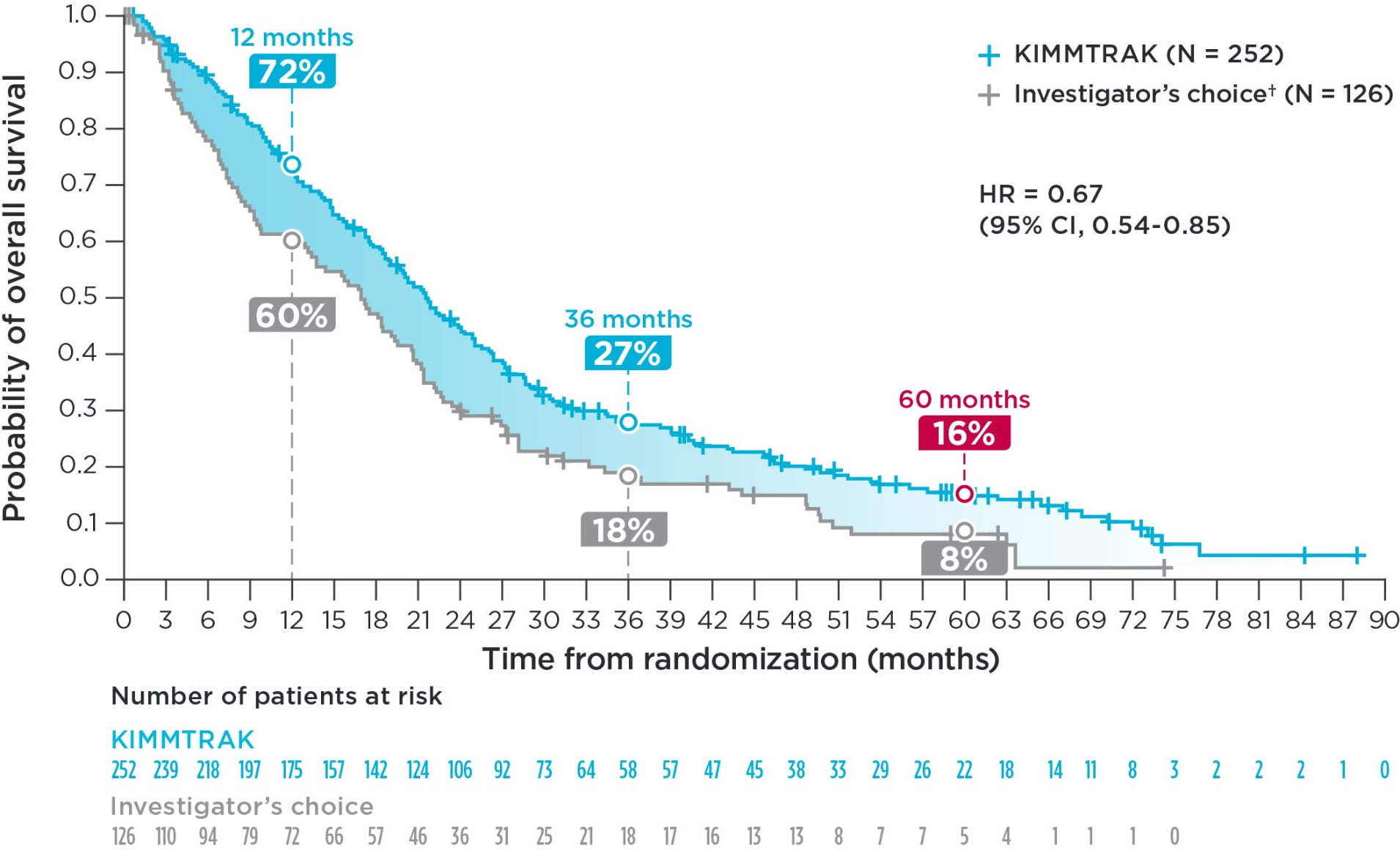
Patients assigned to KIMMTRAK showed a long-term survival advantage at 5 years (KIMMTRAK median overall survival 21.6 months [19.0-24.3] vs 16.9 months [12.9-19.5] with investigator’s choice, 95% CI).2
As of July 2, 2025, all study participants had the opportunity for at least 60 months of follow-up, with a median follow-up of 62.4 months.2
Of the patients surviving at least 5 years2,10:
- 44% (11 of 25) in the KIMMTRAK arm reported ONLY receiving KIMMTRAK
- 86% (6 of 7) in the control group received subsequent KIMMTRAK
The planned exploratory 5-YEAR overall survival analysis occurred after the protocol-specified final analysis and was not tested for statistical significance. No statistical conclusions can be drawn.
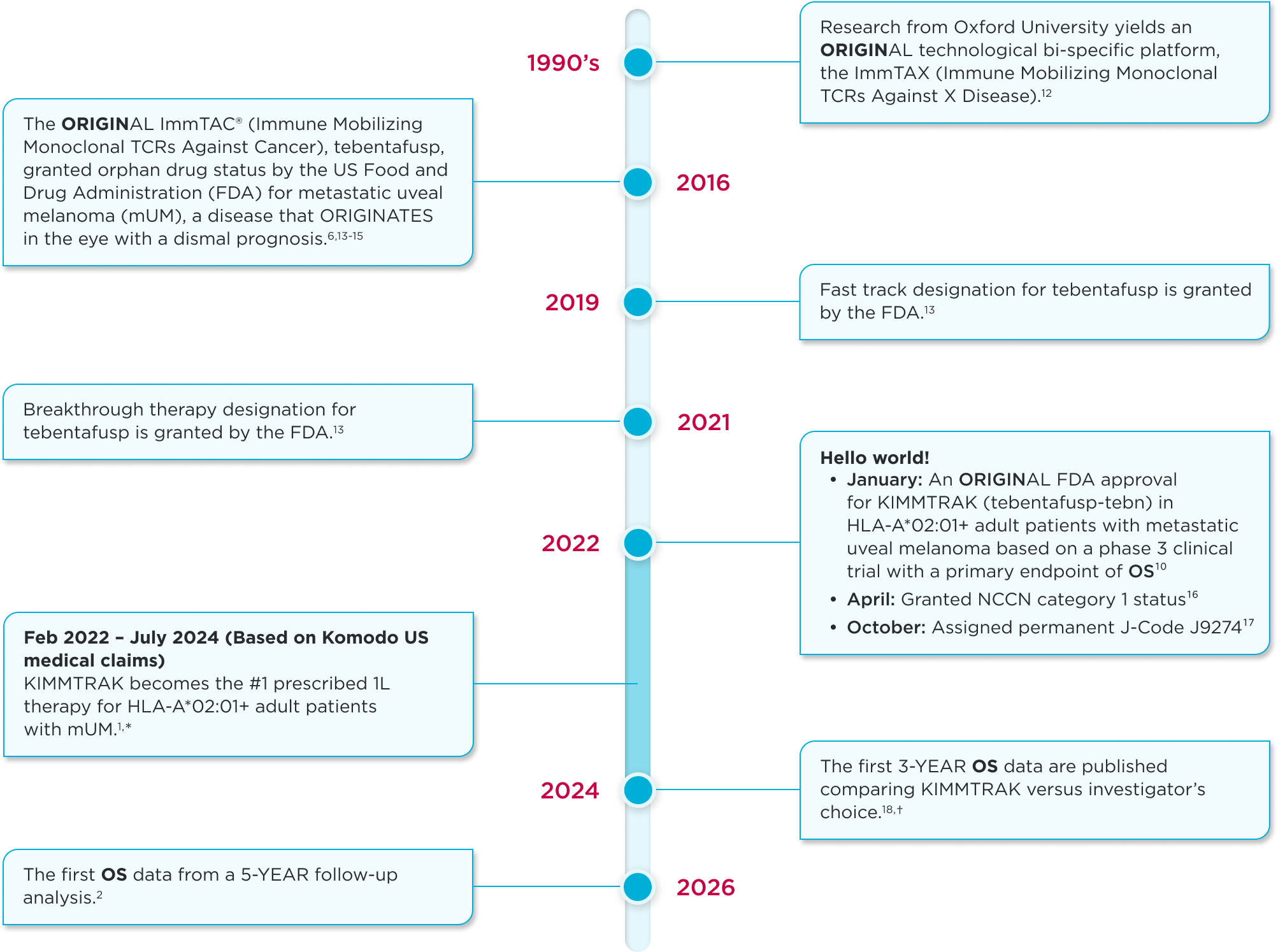
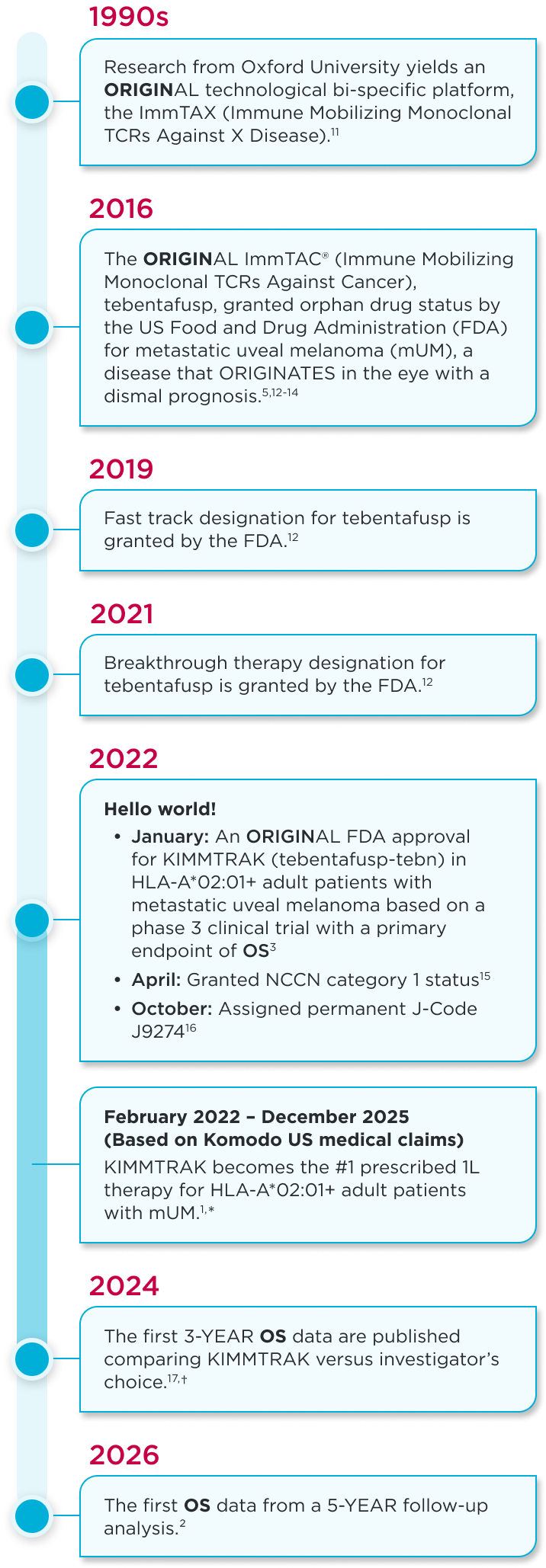
THE KIMMTRAK ORIGIN STORY
CI, confidence interval; HLA, human leukocyte antigen-A; HR, hazard ratio; IC, investigator's choice.
Mechanism of action
A first-in-class T cell engager directed against mUM3
- KIMMTRAK is an ImmTAC‡ molecule that targets gp100, an intracellular antigen presented on the cells of HLA-A*02:01-positive patients with mUM3,4,18
- KIMMTRAK binds to the gp100/HLA-A*02:01 complex to form an immune synapse, which activates cytotoxic T cells that target and kill gp100-expressing UM tumor cells3,19,20
- Normal melanocytes could also be targeted20
- KIMMTRAK has 1 million-fold greater affinity for gp100 presented by HLA-A*02:01 than natural T cell receptors19,21
- T cell engager directed against mUM based on in vitro and in vivo studies3,20,22
- *Based on Komodo US medical claims from February 2022-December 2025 and calibrated with actual vials sold.1
- †Investigator’s choice included checkpoint inhibitors (pembrolizumab and ipilimumab) or chemotherapy (dacarbazine).2-4
- ‡ImmTAC (Immune Mobilizing Monoclonal TCRs Against Cancer) molecules are bispecifics comprised of a T cell receptor targeting domain and an effector function pioneered by Immunocore.3
CI, confidence interval; HLA, human leukocyte antigen-A; HR, hazard ratio; IC, investigator's choice;
mUM, metastatic uveal melanoma; UM, uveal melanoma.
Consider a blood test for your patients with mUM to determine their HLA status and if KIMMTRAK is right for them.10 Click here to learn more.
Indication
Important Safety Information Including Boxed Warning
KIMMTRAK is indicated for the treatment of HLA-A*02:01-positive adult patients with unresectable or metastatic uveal melanoma.
WARNING: CYTOKINE RELEASE SYNDROME
Cytokine Release Syndrome (CRS), which may be serious or life-threatening, occurred in patients receiving KIMMTRAK. Monitor for at least 16 hours following first three infusions and then as clinically indicated.
Indication and Important Safety Information Including Boxed Warning
Indication
KIMMTRAK is a bispecific gp100 peptide-HLA-directed CD3 T cell engager indicated for the treatment of HLA-A*02:01-positive adult patients with unresectable or metastatic uveal melanoma.
Important Safety Information Including Boxed Warning
WARNING: CYTOKINE RELEASE SYNDROME
Cytokine Release Syndrome (CRS), which may be serious or life-threatening, occurred in patients receiving KIMMTRAK. Monitor for at least 16 hours following first three infusions and then as clinically indicated. Manifestations of CRS may include fever, hypotension, hypoxia, chills, nausea, vomiting, rash, elevated transaminases, fatigue, and headache. CRS occurred in 89% of patients who received KIMMTRAK with 0.8% being grade 3 or 4. Ensure immediate access to medications and resuscitative equipment to manage CRS. Ensure patients are euvolemic prior to initiating the infusions. Closely monitor patients for signs or symptoms of CRS following infusions of KIMMTRAK. Monitor fluid status, vital signs, and oxygenation level and provide appropriate therapy. Withhold or discontinue KIMMTRAK depending on persistence and severity of CRS.
Skin ReactionsSkin reactions, including rash, pruritus, and cutaneous edema occurred in 91% of patients treated with KIMMTRAK. Monitor patients for skin reactions. If skin reactions occur, treat with antihistamine and topical or systemic steroids based on persistence and severity of symptoms. Withhold or permanently discontinue KIMMTRAK depending on the severity of skin reactions.
Elevated Liver Enzymes Elevations in liver enzymes occurred in 65% of patients treated with KIMMTRAK. Monitor alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total blood bilirubin prior to the start of and during treatment with KIMMTRAK. Withhold KIMMTRAK according to severity.
Embryo-Fetal ToxicityKIMMTRAK may cause fetal harm. Advise pregnant patients of potential risk to the fetus and patients of reproductive potential to use effective contraception during treatment with KIMMTRAK and 1 week after the last dose.
The most common adverse reactions (≥30%) in patients who received KIMMTRAK were cytokine release syndrome, rash, pyrexia, pruritus, fatigue, nausea, chills, abdominal pain, edema, hypotension, dry skin, headache, and vomiting. The most common (≥50%) laboratory abnormalities were decreased lymphocyte count, increased creatinine, increased glucose, increased AST, increased ALT, decreased hemoglobin, and decreased phosphate.
Please see full Prescribing Information, including BOXED WARNING for CRS.